Reducing Impulsive Sound
Due to Airbag Deployment
in a Passenger Car
Robert Hickling - sonomet@aol.com
Sonometrics, Inc.
8306 Huntington Rd.
Huntington Woods, MI 48070
(248)545-2789
Kathleen Yaremchuk MD, kyaremc1@hfhs.org
Henry Ford Health System
Dept. of Otolaryngology
2799 West Grand Blvd.
Detroit, MI 48202
Gary Newton, Jr., gary.newton@bksv.com
Bruel & Kjaer Sound and Vibration Measurement A/S
15873 Middlebelt Road
Livonia, MI 48154
(734)522-1526
Popular version of paper 3pNS6
Presented Wednesday Afternoon, December 4, 2002
First Pan-American/Iberian Meeting on Acoustics, Cancun, Mexico
A review is presented of the overpressure and noise due to airbag deployment in a passenger car. Overpressure is the low frequency compression of the air in a closed compartment, and noise is the higher frequency sound of bag inflation. Such a review is timely, because there is now an accumulation of medical evidence to indicate that the overpressure and noise resulting from airbag deployment can be a threat to hearing, while, at the same time, the growing use of multiple airbag systems increases the threat. The problem can be counteracted by using aspirating airbags that draw in air from the passenger compartment. There are two types of aspirating bag: one using suction that requires a compartmentalized bag structure and the other using entrainment that does not require a compartmentalized bag. To date use of a compartmentalized bag structure has been avoided. However the bag that appears to be most effective is one with a compartmentalized structure, originally developed at GM, that draws in air from the passenger compartment as it deploys. Results reported here show that this airbag provides a sufficient restraining force while reducing overpressure and noise significantly. In addition the compartmentalized structure provides other safety features. The relative merits of suction and entrainment are discussed in the paper. SAE standard J247 lists the requirements for accurate measurement of overpressure and noise due to airbag deployment. Instrumentation that satisfies these requirements has been developed by Bruel & Kjaer and is described in the paper.
Medical Evidence
Airbags are known to be effective in reducing death and serious injury to vehicle occupants in crash situations, especially when used in conjunction with seat belts [1]. However there is an unavoidable side effect in that airbag deployment may be injurious to hearing. In early experiments with human volunteers [2], it was concluded that this was not a threat to hearing. However the level of impulsive sound associated with airbag deployment is quite high, and comparable to levels known to cause hearing loss in other situations, such as gun blast. It is not surprising, therefore, that later reports by physicians in the USA and Europe [3-8] showed that airbag deployment can in fact injure the hearing systems of susceptible individuals. Table 1 provides a summary of recent case histories.
TABLE 1. Data relating to Patients with Otologic Symptons resulting from Airbag Deployment
| Male | 26 |
| Female | 40 |
| Average Age | 51.5 years |
| Age Range | 4 to 81 years |
| Tinnitus (permanent) | 52 |
| Unilateral Hearing Loss | 47 |
| Vertigo | 13 |
| Recruitment | 6 |
| Perforation of the Tympanic Membrane | 6* |
| Perilymph Fistula | 1 |
| Benign Paroxysmal Positional Vertigo | 7 |
Definitions:
Tinnitus - Ringing in the ears. It can be transient or permanent, unilateral
or bilateral.
Vertigo - Dizziness
Recruitment - A phenomenon where raising the sound level by a small amount
results in it being perceived as excessive and uncomfortable.
Tympanic Membrane - Eardrum. This ruptures when exposed to sound pressure
levels of about 180 dB or more.
Perilymph Fistula - Rupture of the oval window in the middle ear. This
results in chronic dizziness.
Benign Paroxsymal Positional Vertigo - Episodic dizziness associated
with displacement of the otoliths in the semicircular canals. Benign means it
is not life threatening.
Engineering Solutions
Engineering effort to reduce the risk of injury to hearing is constrained by the fact that airbags have to be in place fast enough to prevent crash victims from impacting the hard interior surfaces of the vehicle. Hence some degree of overpressure and noise is unavoidable. Methods of reducing overpressure and noise were investigated in an early paper [9], the most effective being a compartmentalized aspirating airbag originally developed at GM [10] that draws in air from the passenger compartment, reducing overpressure by reducing the amount of displaced air, and reducing noise by using less inflation gas. The outer inflated structure of the original prototype bag resembles a side-by-side arrangement of annuli or doughnuts while the inner cavity is cylindrical with cloth flapper valves at each end. The volume of the bag is divided equally between the outer inflated structure and the inner suction cavity. This prototype was tested on a sled, with a pendulum simulating the impact of a vehicle occupant in a crash. The purpose of the test was to demonstrate that enough ambient air was drawn into the inner cavity to act as part of the restraint on the vehicle occupant. This is apparent from the sequence of stills shown in Figure 1.
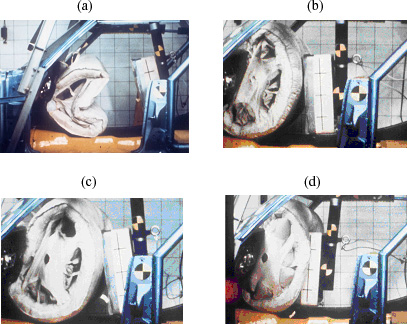
Figure 1. Movie stills of a sled test of the prototype compartmentalized aspirating airbag, with a pendulum simulating the impact of a vehicle occupant
As the bag deploys the cloth flapper valves on the sides connecting to the inner cavity are open, drawing in ambient air. Then, when the pendulum impacts the bag, the air pressure in the inner cavity becomes positive, closing the valves and preventing the ingested air from escaping, as shown by the cloth valves bulging outwards. In this way the air in the inner cavity acts as part of the restraining force of the bag, in addition to the inflated outer tubular structure. The prototype bag in Figure 1 is not the right shape for a vehicle. A more appropriate shape, suitable for a front seat passenger [10], is shown in Figure 2. This bag was tested in a
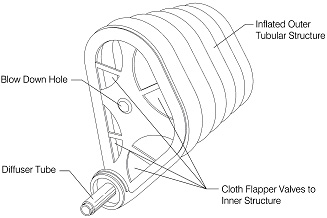
Figure 2. Drawing of compartmentalized aspirating airbag for a front seat passenger
closed compartment, as reported in Reference 9. The difference in the sound pressure pulse between this bag and a regular bag of the same volume is shown in Figure 3.
(a) 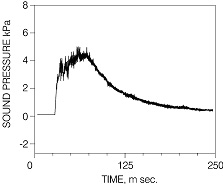 (b)
(b)
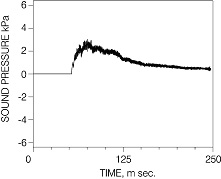
Figure 3. The pressure pulse due to deployment in a closed compartment of the aspirating bag in Figure 2 compared to the pressure pulse of an ordinary bag of the same shape and volume: (a) ordinary bag, (b) aspirating compartmentalized bag.
Both the low frequency overpressure and the higher frequency noise riding on the overpressure are reduced by about 6 dB or more. A reduction of this amount significantly reduces the number of people whose hearing could be affected [9].
There is another method of aspiration, based on entrainment rather than on suction, that does not use a compartmentalized bag. Gas flowing from the inflator can entrain ambient air as it enters the bag. In this way air is drawn into the bag, mixed with gas from the inflator. The entrainment method has been tested, apparently with some success, but other unpublished reports indicate little success. In recent tests, the amount of entrained air was measured to be 7.8 %, whereas the volume of ingested air for the suction airbags just described, is estimated to be almost the same as the volume of gas from the inflator. Also there would seem to be an inherent problem with the entrainment method because the air intake is located at the inflator and instrument panel where some extraneous object or even the bag itself may foul the entrainment. In contrast the air intake for the suction method can be anywhere on the bag. Hence the entrainment method may not always be effective, whereas the effectiveness of the suction method is clearly demonstrated here.
In addition to reducing overpressure and noise, compartmentalization of the bag has some inherent safety features. These are:
(a) Gas from the inflator at the instrument panel is directed up and down to inflate the outer tubular structure of the bag, and the initial deployment of the bag is not directed towards the vehicle occupant. This is an important feature, particularly if the occupant is out of position and in the path of the airbag.
(b) Compartmentalization introduces the air mattress effect. If the bag is only partially inflated, a vehicle occupant is less likely to "fall through" the tubular structure and impact a hard surface underneath.
References
1. National Highway Traffic Safety Association, Safety Fact Sheet, 1998.
2. Nixon, C. W., "Human Auditory Response to an Airbag Inflation Noise", Final Report, DOT Contract Number P. O. 9-1-1151,1969.
3. Kramer, M. B., Shattuck, T. G. and Charnock, D. R. "Traumatic Hearing Loss following Airbag Inflation", New Engl. J. Med., Vol. 337, 574-575, 1997.
4. Saunders, J. E., Slatter, W. H. and Luxford, W. M., "Automobile Airbag Impulse Noise: Otologic Symptoms in Six Patients", Otolaryngology- Head and Neck Surgery, Vol. 44, 238-239, 1998.
5. McFeely, W. J. Jr., Bojrab, D. I., Davis, K. G and Hegyi, D. F., "Otologic Injuries caused by Airbag Deployment", Otolaryngology-Head and Neck Surgery, Vol. 121, 367-373, 1999.
6. Yaremchuk, K. and Dobie, R.A., "The Otologic Effects of Airbag Deployment", Journal of Occupational Hearing Loss, Vol. 2, Nos. 2 and 3, pp 67-73, 2000.
7. Klask, J., "Injuries of Ear, Nose and Throat caused by Airbag Deployment", Laryngo-Rhino-Otologie, Vol. 80, 146-151, 2001.
8. Yaremchuk, K. and Dobie, R. A., "Otologic Injuries from Airbag Deployment", Otolaryngology-Head and Neck Surgery, Vol. 125, No. 3, 130-134, 2001.
9. Hickling, R., "The Noise of the Automotive Safety Air Cushion", Noise Control Engineering, Vol. 6(3), pp. 110-121, 1976.
10. Fleck, L. L. and R. Hickling, "Occupant Restraint Cushion", U.S. Patent, No.3,784,225, Jan 1974.