Hospital Noise and Its Effects on Staff
Timothy Y. Hsu - gth776e@mail.gatech.edu
Erica E. Ryherd - Erica.ryherd@me.gatech.edu
Georgia Institute of Technology,
James West - jimwest@jhu.edu
Colin Barnhill - colinbarnhill@gmail.com
ECE Department
Marie Swisher - swishma@jhmi.edu
Weinberg 5D- Medical Oncology,
401 N. Broadway
Natalia Levit - Natalia.V.Levit@usa.dupont.com
DuPont Corporation
Spruance Plant
Popular version of paper 2aNSc8
Presented Tuesday morning, April 20, 2010
159th ASA Meeting,
Introduction and
Background
We have all experienced excessive noise in our lives -- whether it is in the office place, in a classroom, or at a parties. Most people find this excessive noise to be just a nuisance. However, over a prolonged period, it is not hard to imagine that excessive noise can affect how you work, how you concentrate, and possibly even how your body functions. Our research focuses on the soundscape of hospitals. Some of our research questions are: 1) How loud are hospitals? 2) What is the best way to describe the noise in hospitals? 3) How does noise affect the staff and patients both psychologically and physiologically? 4) How can we design hospitals better?
Hospital sound environments consist of various different types of sources including occupants, equipment, and other environmental sources. Two general acoustic factors of interest are background noise levels and reverberation time. Reverberation time reveals how long the ward echoes. One can imagine that a large gothic cathedral is going to echo much longer than an elementary school classroom. To control this reverberation time, acousticians can add acoustical absorptive products to absorb the echoes or sound reflections.
Hospital soundscape research is still in its preliminary
stages. The research being presented here
is based on a collaboration between
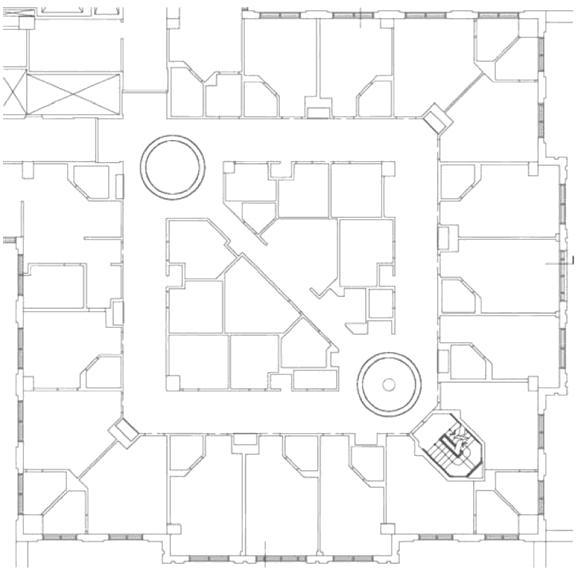
In this study, we focused on a comparison study where the primary difference between the two wards was the acoustical treatment. The wards are denoted by the floor level and a letter. The floorplan for the ward is shown in Figure 1. Ward 5A was treated with DuPont Tyvek material over fiberglass panels. The panels were installed on the upper walls and ceilings of the corridors and in the domes above the central nurse stations. The panel surface area comprised approximately 30% of the total surface area in the corridors. 5D was left untreated, with no acoustical absorption added. In the acoustic comparison, this study compares a treated 5A with the untreated 5D.
As a follow-up, a twenty-question paper questionnaire was developed for the registered nurses to determine their perception of the sound environment. They were asked about noise sources -- if they heard particular noises, if the noise affected them, and if they experienced a particular type of reaction due to a particular noise. In the closed-ended response section a 5-point scale was used. For example, they were asked to what degree (from Not at all to A great deal) noise contributed to some physiological symptom such as headache or tiredness. In this portion of the study, a comparison is made between 5A before the treatment to 5A after the treatment was installed.
Results
A. Acoustic measurement
results
1. Background noise results
As previously stated, ward 5A was treated with added acoustic absorption whereas 5D was untreated with primarily hard surfaces. Comparing the average A-weighted equivalent sound pressure level, LAeq, at multiple locations in each ward, these results show elevated noise levels in both wards that exceed the World Health Organization (WHO) standards. The WHO standards state that Leq in a patient room should not exceed 35 dBA during the day, 30 dBA at night, and that the A-weighted maximum sound pressure level (LAmax) should not exceed 40dBA at night. Moreover, direct comparisons can be made between the untreated ward and the treated ward. For example, in the treated 5A ward, a 4 dB reduction in LAeq was found at the front nurse station. The other locations in the treated 5A ward were also generally quieter than the untreated 5D locations, with roughly a 3 dB difference in LAeq in all of the locations. These differences in sound level are great enough to be generally noticeable to the occupants.
Several standardized different indoor noise criteria were also calculated using sound levels across frequency. At nearly all locations measured, the treated ward yielded a quieter noise metric than the untreated wardthereby showing that the addition of these absorbing sound panels have had a positive impact on the noise soundscape.
2. Reverberation time results
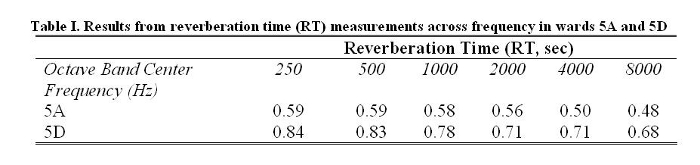
Table I shows the octave band reverberation times averaged across multiple trials in both wards. As expected, the untreated 5D ward has a longer RT in almost all frequency ranges. For example, at 500 Hz RT was reduced by 0.24 seconds, or 29%.
B. Questionnaire
results
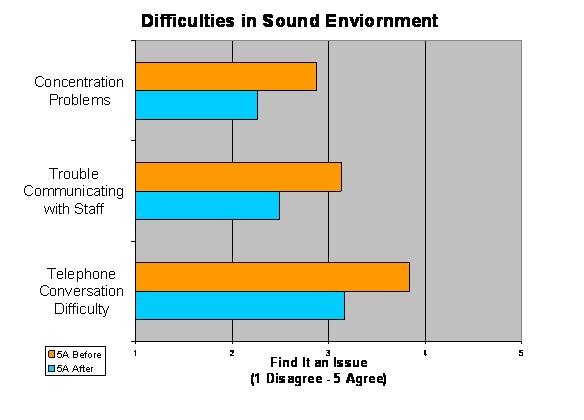
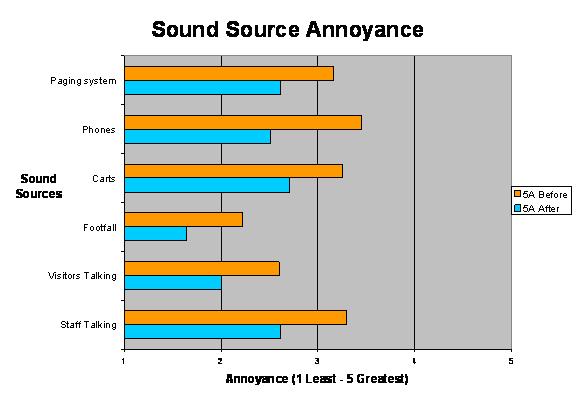
Comparing the questionnaire results from 5A before the treatment to 5A after the treatment, all the question results showed trends of improvement in perception of the treated ward. Moroever, many questions showed statistically significant differences. Specifically, in the treated ward, the nurses were less bothered by talking noise, rolling cart noise, footfall noise, and phone/pager rings. They also reported that they had more problems with speech communication and concentration in the untreated wards. These results can be seen in Figure 2 and Figure 3.
Conclusion
This study evaluated the impact of adding acoustical absorption to a hospital ward. Specific comparisons between untreated wards and a ward treated with absorbing panels were made. The data presented shows improvements in background noise, noise metrics, and reverberation time. Additionally, there was a consistent trend of positive improvement from the untreated to the treated ward with the questionnaire results. It is concluded that the addition of these sound absorbing panels improved the soundscape of these wards.
The reverberation time was also improved when absorbing panels were installed. Perceptually, the installed sound panels have created a noticeable change in RT in the treated ward. Reverberation time can be linked to speech intelligibility, or how well you can hear the words being spoken. Generally, with longer reverberation times, the speech becomes harder to understand. One concern in a hospital with poor speech intelligibility is that the risk for medical errors caused by miscommunication can rise. Two ways to improve speech intelligibility is to reduce the background noise and to reduce reverberation time -- both of which were achieved in this study.
All of these acoustic results are reinforced by the questionnaire results. Even though not all questionnaire comparisons were statistically significant, all survey results showed a trend towards improved perception ratings in the treated ward as compared to the untreated ward. Focusing on the statistically significant results, it is seen that the questions that focused on activities in the hallways and working areas were generally significantly different; whereas, the questions that focused on activities in the patient rooms were not statistically different. This is important because the acoustic panels were only installed in the hallways and working areas, and not in the patient rooms. This again emphasizes that these panels are making a measurable difference to the staff members in these wards.
It is our hope that this research can provide a better working environment for staff members of the hospitals and that future hospitals can be designed with this research in mind.