Bryan W. Cunitz (1) – bwc@apl.washington.edu
Barbrina L. Dunmire (1) – mrbean@u.washington.edu
Mathew D. Sorensen (2, 3) – mathews@uw.edu
Franklin Chong-Ho Lee (2) – franklee@u.washington.edu
Ryan His (2) – rshsi@u.washington.edu
Oleg A. Sapozhnikov (1, 4) (1) – olegs@apl.washington.edu
Jonathan D. Harper (2) – jdharper@u.washington.edu
Michael R. Bailey (1, 2) (1, 4) (1) – bailey@apl.washington.edu
(1) Center for Industrial and Medical Ultrasound, Applied Physics Laboratory, University of Washington, USA
(2) Department of Urology, University of Washington School of Medicine, USA
(3) VA Puget Sound Health Care System, USA
(4) Department of Acoustics, Physics Faculty, Moscow State University, Russian Federation
Popular version of paper 1aBA5
Presented Monday morning, December 2, 2013
166th ASA Meeting, San Francisco
SIGNIFICANCE
The novel stone-specific ultrasound technology we are developing has the potential to revolutionize care for the 3 million stone patients in the United States who will seek emergent medical treatment each year and the nearly 30 million Americans who will suffer a stone event in their lifetime. This technology will dramatically expand options for the noninvasive removal of stones, allowing doctors to precisely localize and accurately determine stone size without ionizing radiation, move problematic renal stones to a favorable location for surgical treatment, deliver small stones and residual fragments to the uretero-pelvic junction to speed passage down the ureter, and relieve urinary obstruction to avoid aggressive emergency intervention.
This new ultrasound-based stone therapy system is composed of two main elements delivered in the same hand-held ultrasound (US) transducer. The ultrasonic propulsion (UP) component functions on the principle of acoustic radiation force to generate a targeted force to push and guide stones. The imaging component (S-mode) is the first ultrasound mode specifically designed to image kidney stones with automated features to make stone imaging less dependent on operator skill. It incorporates new technology to identify stones in a high contrast harmonic B-mode and to improve the size measurement of even very small stones. The system's stone detection technologies also enable cavitation feedback during treatment for stones.
The system is visual, intuitive, user friendly, and requires minimal training. The user images the stone with the US probe, assesses the path for stone expulsion, touches the touch-screen, and monitors stone motion in real time. The user navigates the stone through the collecting system, pushing the stone in a series of ~1 cm skips and hops. The entire procedure and can be performed in an office setting, without anesthesia. These applications will improve patient stone-free outcomes. Periodic elective removal of incidental stones will keep patients stone-free and symptom-free longer. Costly invasive surgical interventions will be reduced, and recurrent stone formers will receive significantly less exposure to radiation over the course of their disease.
INNOVATION
1. S-mode is the first stone-specific ultrasound modality. Indeed, S-mode consists of a suite of novel US modalities we are developing to specifically localize, identify, target, and measure urinary stones and will be applied for the first time to an array of currently available surgical stone interventions.
2. Stone detection by ultrasound can be made highly sensitive and automated. We discovered bubbles cause twinkling and have implemented modified US transmission and processing to accentuate this response. The result is a stone-specific signature that enables the machine to identify where in the image the stone is located.
3. Stone tracking in real-time to improve the efficiency of shockwave lithotripsy is readily achievable using S-mode. S-mode enables accurate targeting of therapy waves from shockwave lithotripsy to the stone, and not in the surrounding tissue, as the target moves with the patient's respiration.
4. Ultrasound determination of stone size comparable to the resolution of CT. We have found the stone's posterior acoustic shadow gives an accurate measure of stone size, and as such, have programmed S-mode to automatically enhance the contrast of the shadow.
5. Ultrasonic propulsion (UP) is the only noninvasive means to manipulate stones within the kidney and has the potential to relieve acute urinary obstruction. A probe against the skin and touch-screen control allows a user to confirm a stone by nudging it, steer a stone out of the kidney, and more.
APPROACH
Background to ultrasound imaging of stones: In an example recent year (2007), 72 million CT exams were conducted in the U.S., and in a 2011 study, radiation from CT exams related to stone disease alone exceeded the total radiation dose limit established by the International Commission on Radiological Protection in 38% of kidney stone patients. The FDA and AUA (American Urological Association) have reacted with calls to reduce CT exposure and have introduced certification courses on the use of non-ionizing US imaging, which urologists have embraced with over 1000 already certified. US is a noninvasive, portable, non-ionizing, inexpensive imaging modality available worldwide. US is the standard in many applications, including, for example, obstetrics and vascular imaging.
For the management of kidney stones, ultrasound is underutilized, particularly in the United States, for three main reasons: low sensitivity and specificity in stone detection, inaccuracy in stone size determination, and operator dependence. For example, false positive stones found on ultrasound can lead to unnecessary surgeries. Technical factors contribute to exacerbate these limitations in larger patients. In addition, US is a modality best viewed real time and interpreted by the operator holding the probe and aware of its position, not in the radiology report. However, in current practice in the United States, most patients with kidney stones are sent out to radiology facilities, and the managing physician decides treatment based on a radiology report.
Our advances to ultrasound imaging of stones: We have developed and implemented custom algorithms on a software based US system to address the limitations described above. We have developed a more sensitive and specific stone detector. The system more accurately measures stone size. Many features have been automated to reduce user dependence. We include system testing at large depths to address challenges patients who have larger skin-to-stone distances. The entire suite of functions is referred to here as stone-specific mode or S-mode.
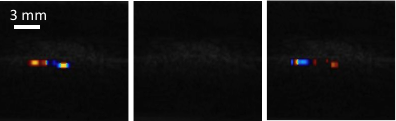
S-mode is developed from evidence that twinkling artifact is caused by bubbles. Twinkling artifact is intermittent color that may appear on kidney stones imaged with Doppler ultrasound. Bubbles can be suppressed by hyperbaric pressure and similarly we found twinkling was suppressed as shown in Fig. 1.
Fig. #1: Results from a hyperbaric experiment on an excised porcine kidney containing naturally occurring (diet-induced) stones: (left) twinkling at ambient pressure. (center) no twinkling at elevated pressure (threshold 4-9 atm), (right) twinkling on return to ambient pressure. Studies with human stone patients in a hyperbaric chamber are underway.
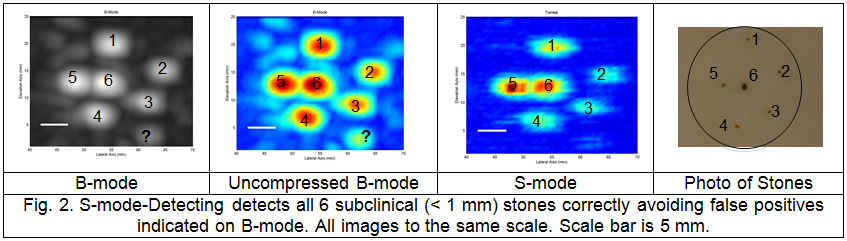
S-mode has been shown to reduce or eliminate false positives detected in standard B-mode imaging in human subjects and as shown in Figure 2 in even very small kidney stones in vitro.
Background to current limitations of therapy for stone disease: Kidney stones are one of the most common and painful urological disorders around the world. The global prevalence and incidence of renal calculi is reported to be increasing. One in 11 Americans suffer from kidney stones at an annual economic burden of $5 billion, in part from recurrence and repetitive treatment and monitoring. All minimally invasive therapies to treat stones have the potential to leave residual stones or fragments, which may grow and require retreatment in up to one-fifth of patients with long-term follow-up. Small asymptomatic stones that are observed rather than treated may also ultimately require intervention. Likewise, patients presenting with an acute obstructing stone may be accompanied by signs of infection, hemodynamic instability, renal insufficiency, or intractable nausea or pain. Currently, the only options to relieve obstruction are surgical. As a result, stone management often entails a long repetitive cycle of follow-up visits, monitoring, medication courses, and even surgeries when the goal is intuitively to be stone free as soon and as simply as possible.
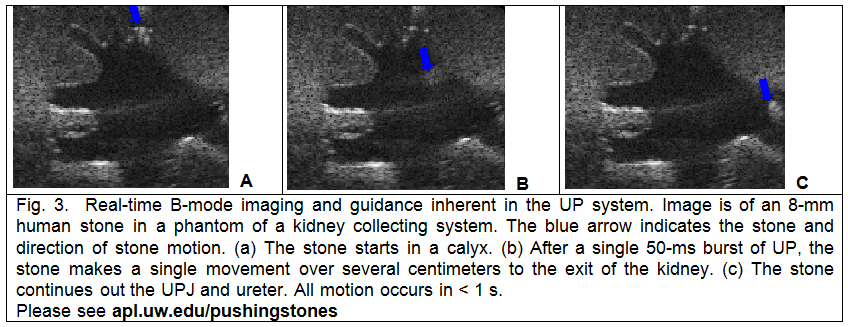
Our advances on current limitations of therapy for stone disease: We have developed, implemented, tested, and received an investigational device exemption (IDE) for the ultrasonic propulsion (UP) of kidney stones. Using the same diagnostic transducer and system as S-mode, a stone may be repositioned within the kidney or pushed to the ureter. The transfer of momentum from the acoustic wave to the stone displaces the stone in situ by about 1 cm. Figure 3 shows a stone repositioned by UP in a kidney phantom. UP has proven to be safe and effective in animals and feasibility testing is currently underway in human subjects.