Acoustical Society of America
ICA/ASA '98 Lay Language Papers
Can a Machine Outperform a
Radiologist in Interpreting Ultrasound Images?
- Hope for a Cheap and Reliable Automatic Diagnostic
System for Breast Cancer! *
Georgia Georgiou - ggeo@cbis.ece.drexel.edu
Fernand S. Cohen - fscohen@coe.drexel.edu
ECE Dept., Drexel University, 32nd and Chestnut Streets
Philadelphia, PA 19104
Popular version of paper 5aSP5
Presented Friday morning,
June 26, 1998
ICA/ASA 98, Seattle, WA
Ultrasound is in general a safe and low cost medical imaging technique, with most of the cost being the radiologist's time for examining the ultrasound image. Unfortunately there are some problems associated with it that make its use as a reliable mean for early breast cancer detection quite limited. Several clinical studies have shown that ultrasound is rather incapable of reliably detecting cancers in the breast that were not also evident by physical examination or mammography. This happens because the use of ultrasound imaging of the breast is still based on the radiologist who observes the images. The extracted visible information is limited because of the relatively low resolution of the imaging system. Unfortunately, the resolution can not be increased due to the tradeoff between the resolution of a specific ultrasound imaging system and the depth of penetration that it can achieve. In other words, because we need to examine organs more than 3 cm thick we have to accept a rather small resolution of the imaging system. Moreover there is a masking effect of the non-resolvable scatterers of the breast tissue to the resolvable ones that decreases the quality of the image even more. This work attempts at extracting parameters that relate to the structure of the breast, and using them for examining the tissue for early signs of cancer. These parameters can be arrived at by tracking down the interaction of the transducer pulse (the imaging device) with the organ being imaged.
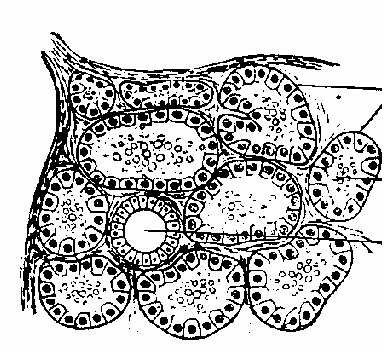
Fig. 1: Schematic diagram of the breast tissue.
If we examine the schematic diagram of the breast tissue that appears in Fig. 1., we can observe the following. The breast tissue is organized in lobes and these are composed of lobules which are arranged in a quasiperiodic manner and are connected together by areolar tissue, blood vessels and ducts (the circular object in the center). If we take under consideration the size of the ducts (which is comparable with the size of the lobules) and the imaging formation process, we conclude that the echoes of the fat-ducts boundaries and the fat-lobules boundaries as well, are resolvable with the usual ultrasonic techniques in use today. What remains left, are the fat cells that occupy the interior of the lobules and the space between the lobes. These scatterers produce the non-resolvable part (known as speckle) of the ultrasonic breast signal which by and large is the component responsible for the masking effect that prevents a clear visual examination of the ultrasound image.
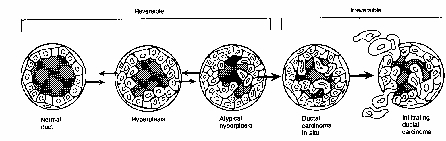
Fig. 2: Cancer appearance in the breast tissue.
Almost 90% of the cancer tumors originate in the ductal epithelium. When cancer starts to appear, the ductal epithelium undergoes hyper-plastic growth (as seen in Fig.2). The duct is filled with cells of various sizes and shapes. As the cancer grows the quasi-periodic structure of the cancer is destroyed.
Our work aims at decomposing the radio-frequency ultrasound signal into two components. The first component (the coherent component) is due to the resolvable scatterers of the breast (ducts and lobules) and the second component (the diffuse component) is due to the non-resolvable scatterers. This decomposition is consistent with the tissue microstructure and allows us to model each component separately. Parameters related with the tissue structure such as the mean average spacing, the strength of the coherent part, etc. can be estimated. By using a sliding window we were able to produce parametric images in which the lesion has a better contrast than the initial radio-frequency image. Parametric images of the diffuse scatterer density (number of diffuse scatterers per resolution cell) and the coherent scattering strength are displayed in Fig 3.b and 3.c. The original radio-frequency image that contains a cancerous lesion appears in Fig 3.a (logarithmically compressed for better displaying).
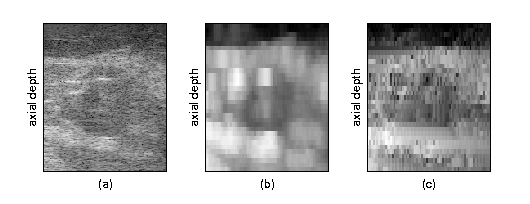
Fig. 3: Parametric images.
The same parameters can be used as features for cancer detection and for differentiating between benign and malignant cases. The database of images that we used contained 370 B-scan images from 52 patients, obtained in the Radiology department of the Thomas Jefferson Hospital. The pathologies of interest are carcinoma fibrocystic and stromal fibrosis disease and fibroadenoma. Empirical receiver operating characteristics (ROC) techniques were used to evaluate the detection rate on single parameters of the model such as the residual error variance and the autoregressive parameters of the diffuse component of the radio frequency echo. The area under an ROC curve quantitatively characterizes the performance of the system under examination. When the area is equal to 0.5 the system is absolutely useless and when the area is close to 1 the performance is excellent. The area under the ROC curve for detecting lesion regions versus normal regions is 0.901. The area under the ROC curve for detecting carcinoma versus normal regions is 0.904. The corresponding areas for normal regions versus stromal fibrosis/fibrocystic regions and fibroadenoma regions are 0.942 and 0.899 respectively.
In conclusion we would like to state that the Wold decomposition that was developed in our laboratory in Drexel University is consistent with the breast tissue microstructure and thus can detect changes in the tissue that are not visually seen. We produced parametric images that enhance a malignant or benign tumor relatively to the surrounding tissue. The performance of the algorithm was measured using a large database of real radio-frequency images and empirical ROC curves and found to be very satisfactory.
* This work is supported by the National Cancer Institute and the National Institutes of Health under grant number CA52823.