Acoustical Society of America
159th Meeting Lay Language Papers
[ Lay Language Paper Index | Press Room ]
Ossi Riekkinen - ossi.riekkinen@uef.fi
Janne Karjalainen - janne.karjalainen@uef.fi
Jukka S. Jurvelin - jukka.jurvelin@uef.fi
Department of Physics and Mathematics
University of Eastern Finland
P.O. Box 1627, 70211 Kuopio, Finland
Popular version of paper 5aBB4
Presented Friday morning, April 23, 2010
159th ASA Meeting, Baltimore, MD
At the moment, approximately 200 million people around the world suffer from osteoporosis. A majority of patients with osteoporosis are not diagnosed before low-trauma fractures occur. Therefore, early diagnostics should be rationalized for effective screening of individuals at risk before fractures occur. This would require a cheap, easy-to-use and sensitive technique which could be applied in the primary healthcare level. Our aim is to introduce an answer to this problem by presenting unique dual frequency ultrasound (DFUS) methodology.
I. Introduction
A. Background: Osteoporosis
Musculoskeletal diseases are the most common causes for long-term morbidity, pain and immobility around the world. Osteoporosis is a rapidly growing musculoskeletal disease, and, at the moment, it is estimated that 200 million people around the world suffer from it. In the year 2000 the treatment and hospitalization costs due to the osteoporotic fractures were 36 billion euro within the European Union. By the year 2050, the annual costs will be more than doubled. During the first year after a hip fracture, approximately 20-30% of the patients die.
B. Problem: Diagnostics of Osteoporosis
A majority of osteoporotic patients are not diagnosed until fractures occur. For effective management of osteoporosis, early diagnostics should focus on screening of individuals at risk before fractures occur. This is realistic only if diagnostics can be realized at the primary health care level. Today, a medical doctor makes a referral to a major hospital for X-ray diagnostics of osteoporosis. Then, an axial dual- energy X-ray absorptiometry (DXA) measurement of the bone mineral density (BMD) is conducted (Fig. 1).

Figure 1. Axial dual- energy X-ray absorptiometry (DXA) device for measurement of the bone mineral density (BMD) and a typical whole body scan image. In addition to BMD, the soft tissue composition (amount of bone, muscle and fat tissue) can be analyzed.
In addition to the BMD, bone composition and structure contribute to the total strength of the bone. Therefore, only a moderate prediction for fracture risk can be achieved with DXA. A majority of the low- trauma fractures occur in individuals with normal BMD. DXA devices are mostly available only in hospitals and because of the costs (approximately 100,000 euro per device) and the risks related to radiation dose, even small, these devices are not optimal for screening purposes.
Ultrasound (US) measurements of bone have shown potential for osteoporosis diagnostics and fracture prediction. Current clinically-available devices are able to measure only the peripheral locations, such as the heel, where the ultrasound can go through the bone. This is called a through transmission method. In an axial transmission technique, ultrasound travels along the bone, a method suitable only for measurement of long bones like tibia or radius (Fig. 2).
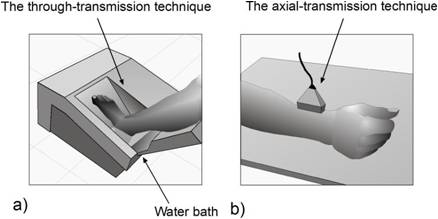
Figure 2. Current commercially-available US devices for osteoporosis diagnostics. Measurement of a) heel in through-transmission and b) radius in axial transmission.
The most severe fracture site in osteoporosis, located at the hip, is challenging for these measurements. The bone properties at the peripheral locations reflect only weakly the bone properties at the central skeleton (e.g. hip). Therefore, the diagnostic value of the devices designed for the measurement of peripheral sites (e.g. heel) is limited. Further, the errors arising from the effects of overlying soft tissue layers on top of the bone (we dont know their thickness or composition) complicate the ultrasound measurements. In fact, the fractures can be predicted most accurately by direct measurements at the fracture site. Therefore, there is a strong and growing need for a reliable, cheap and safe method, applicable at the primary health care level for fracture prediction and osteoporosis management.
C. Solution: Pulse-echo ultrasound
In bone ultrasound measurements, the transducer transmits ultrasound into bone. Part of the sound is transmitted through the bone, but part is echoed (or backscattered) back from bone. Instead of measuring the sound transmission, we quantify the backscattered sound. From this we can calculate pulse-echo parameters that have been shown in laboratory measurements to be strong predictors of the strength of bone samples. In measurements of humans, elimination of the disturbing soft tissue effect is crucial when applying the technique for bone US measurements. In osteoporosis, thickness of the compact bone layer, critical to strength of the long bones (e.g. tibia), also diminishes. Compact bone layer thickness can be measured accurately with pulse-echo US.
We have developed a unique dual frequency ultrasound (DFUS) technique for elimination of the soft tissue effect from the bone US measurement (Fig. 3).
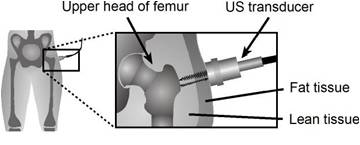
Figure 3. DFUS-based ultrasound method can be used for measurements of the most relevant osteoporotic fracture sites. This was previously impossible. An ultrasound echo from the surface of bone is used for analyzing the composition of soft tissue overlying the bone. With this information the pulse-echo parameters of bone can be corrected to be independent of soft tissue.
With DFUS technique it is possible to measure severe fracture sites such as the hip that have large amounts soft tissue. This was previously impossible. Based on our research results, different bone properties (compact bone and spongy bone) can be analyzed accurately.
With the present ultrasound methodology (Fig. 3) osteoporosis diagnostics and fracture risk prediction may be done using a simple ultrasound system equipped with one ultrasound transducer that acts as a transmitter and a receiver. Diagnostics becomes possible at the primary health care level and unnecessary referrals to hospitals are not needed. The difference between the commercially-available US devices and our technique is obvious (Fig. 2 vs. 3) in terms of measurement geometry and measurement sites. In addition, individuals with high risk for osteoporosis can be measured and intervening medicinal treatments could be initiated for relevant individuals. This completely new concept for management of osteoporosis would diminish the expenses caused by the medical treatments or hospitalization significantly.
II. DUAL FREQUENCY ULTRASOUND TECHNIQUE
A. Theory
The US reflection amplitude at the surface of bone is measured using high and low US frequencies. US pulse is attenuated by overlying soft tissues before and after the reflection (Fig. 3). By analyzing the reflection from the surface of the bone with two frequencies the thickness of lean and adipose tissues can be calculated.
B. Weight loss study
Ultrasound pulse-echo and DXA examinations were conducted on a bodybuilder at above the knee (the distal femur) during a 21-week training and dieting period. The fat mass of the bodybuilder decreased from 20.0 kg to 3.7 kg during the period. Dieting did not affect the BMD values. DFUS technique enabled the determination of local soft-tissue composition, as verified by comparison with the DXA (Fig. 4).
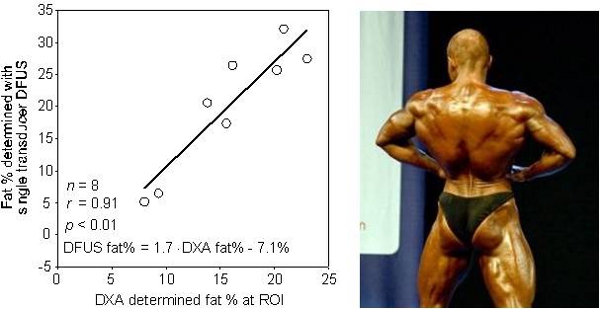
Figure 4. The local soft-tissue composition was determined with DFUS technique and with the present gold standard DXA technique. DFUS was a significant predictor of local soft tissue composition during the dieting period of the bodybuilder.
Further, the technique eliminated the soft-tissue-induced significant error from the pulse-echo parameters measured from the bone.
C. Osteoporotic hip fracture discrimination study
Ultrasound pulse-echo measurements from hip (proximal femur) and upper and lower extremities (radius and tibia) in fractured and healthy patients are currently under examination. The aim of this study is to compare the ability of DXA and ultrasound measurements in discrimination these two patient groups. In the measurements, the DFUS technique will be used for the correction of the soft tissue effects. The compact bone layer thickness is also measured from the long bones (arm and leg) with US.
Preliminary results of 25 patients are encouraging and the pulse-echo ultrasound parameters usefully indicate BMD and discriminate similarly or even better the patients with previous fractures from healthy controls than the DXA.
D. Conclusions
Non-invasive, non-ionizing ultrasound pulse-echo measurements with a unique DFUS technique may be later used for diagnosis of osteoporosis and for prediction of fracture risk of a patient. Then, the properties of compact and spongy bones at the most serious osteoporotic fracture sites (e.g. hip) can be measured. For more reliable prediction of future fractures, information on the clinical fracture risk factors will be combined with ultrasound results to improve the prediction. The ultrasound system will cost about 10% of the price of the DXA devices. It can be easily used in small clinics, maybe even at home. More effective early detection of osteoporosis can produce significant savings for modern societies.