Dual Pulse Lithotripsy Points Toward Faster,
Safer Treatment for Kidney Stones
Dahlia L. Sokolov, Michael R. Bailey, and Lawrence A. Crum - bailey@apl.washington.edu
Center for Industrial and Medical Ultrasound
Applied Physics Laboratory
University of Washington
1013 NE 40th St.
Seattle, WA 98105
James A. McAteer and Andrew P. Evan
Department of Anatomy and Cell Biology
Indiana University School of Medicine
635 Barnhill Dr.
Indianapolis, IN 46202
Popular version of paper 3aBB4
Presented Wednesday morning, December 4, 2002
First Pan-American/Iberian Meeting on Acoustics, Cancun, Mexico
Shock wave lithotripsy (SWL) is a common and effective clinical procedure, in which high-amplitude, focused shock waves, generated outside of the body are used to comminute (fragment) kidney stones. Even with the advent of minimally invasive endourological techniques for stone removal, SWL continues to be the favored method of treatment for uncomplicated, upper urinary tract calculi. However, the evidence is increasingly strong that SWL treatment also causes tissue injury. There is great interest in finding ways to improve the effectiveness and safety of lithotripsy. In the 20 years since the introduction of lithotripsy, over 40 different lithotripters have been developed. Unfortunately, the vast majority, if not all, of these newer models have proven to be less effective at breaking stones than the very first lithotripter introduced to clinical practice. Not only is lithotripsy not improving, but by many clinical measures, treatment outcomes are getting worse. Retreatment rates are higher with new machines, and the incidence of adverse effects is on the rise. Clearly, there is room for improvement.
We tested a new lithotripter design - a dual source, dual pulse lithotripter - that, in laboratory experiments, improves stone fragmentation efficiency and reduces surrounding tissue damage. In lithotripsy, pressure generated inside the stone and cavitation (bubble activity) in the surrounding fluid both play an important role in stone comminution. However, cavitation has been neglected in the design of clinical lithotripters. Our dual pulse system employs two electrohydraulic shock wave generators positioned face to face. They are aligned confocally (i.e. they have the same focus points). Their simultaneous, converging shock pulses localize and intensify cavitation at the focus. Figure 1 shows our lithotripter. At the focus, where the pulses meet, the pressure and cavitation intensity are doubled. Off the focus, the staggered timing of the pulses mitigates cavitation. Thus increased stone comminution with a reduction of surrounding tissue injury may be expected.
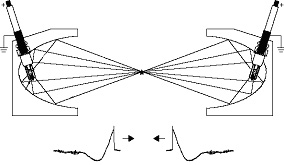
Figure 1: Our dual pulse lithotripter creates two converging pulses that superimpose at a common focus.
In the laboratory, we assessed stone comminution in water and cell damage in suspensions using dual-pulse and conventional single pulse lithotripsy. Two hundred shock pulses from a single lithotripter or 100 pulse pairs from our dual pulse lithotripter at 15 and 18 kV charging voltage and at various axial locations were compared. Cylindrical gypsum stones (6.5x 7.5 mm) were dried, weighed, rehydrated for 48 hours, treated with one of the lithotripters, sifted through a 1.5 mm mesh, dried, and reweighed. The number of fragments and mass loss were recorded. The damage to red blood cells in suspension (10% hematocrit) was measured with spectral absorbance, and was used to model tissue injury.
One hundred dual pulses generated at 15 kV comminuted gypsum stones placed at the geometric focus F2 into 8 times as many fragments (Fig. 2) and significantly reduced hemolysis in dilute blood 2 and 4 cm off F2 when compared to 200 single pulses generated at 18 kV. Thus the dual-pulse lithotripter enhanced comminution and reduced injury while cutting treatment time in half. Additionally, when cavitation was suppressed by placing the stones in glycerol, the improvement in comminution was reduced to only a twofold increase. This result indicates that localized and intensified cavitation is the dominant mechanism in the accelerated comminution produced by the dual pulse lithotripter.
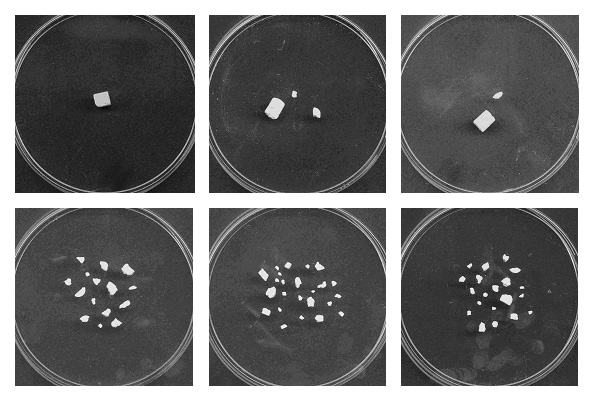
Figure 2: Three stones treated by 200 pulses from a single pulse lithotripter at 18 kV (top) and 100 pulses from our dual pulse lithotripter (bottom).
Dual pulse lithotripsy has the unique potential to enhance stone comminution, reduce tissue injury, and accelerate treatment. Our data point to cavitation control as the key to this potential. There are challenges to clinical implementation of dual pulse lithotripsy, but several research, clinical, and commercial groups have initiated studies to develop dual pulse or cavitation control lithotripters. Our work was supported by NIH grants P01-DK43881 and R01-DK55674.