[ Lay Language Paper Index | Press Room ]
Noise in the Operating Room
Jonathan Kracht jkracht1@jhu.edu, Ilene J. Busch-Vishniac (ilenebv@jhu.edu), and James E. West (jimwest@jhu.edu)
Johns Hopkins University
3400 N. Charles Street
Baltimore, MD 21218
Popular version of paper 4aNS10
Presented Thursday morning, June 8, 2006
151st ASA Meeting, Providence, RI
Very little reliable information exists on the sound levels present in an operating room environment. This information is important because it provides a means of determining the risk of surgery to the hearing of those in the operating room. Further, it is important to assess whether noise in the operating room causes a decline in the quality of speech comprehension because surgery relies on accurate oral communication.
Sound levels were measured in operating rooms throughout Johns Hopkins Hospital (JHH) to quantify the acoustical events during surgical procedures. In total, 38 rooms were measured. Operations in all branches of medicine were examined including neurology, cardiology, orthopedics, urology and plastic surgery. Surgeries performed on both adult and pediatric patients were monitored. Caution was taken to preserve the normal situation for surgery. Surgeons and staff generally were not aware of noise monitoring and no attempt was made to control conversation or other activities during surgery.
A sound level meter was placed inside each operating room for a 24-hour period in an area which did not interfere with the operations occurring. A paper taped to the sound level meter explained that the instrument was present for a study although noise was not mentioned. Other than this notice the medical staff were not informed of the ongoing study in order to avoid changes in operation protocols that might affect the noise. Surgical logs were examined to identify operations occurring within the sampled intervals. The surgery log provides a detailed description of the nature of each procedure and the division of surgery under which it falls. The logs also provide times for surgical events. For each surgery, the total surgery time was assumed to be the time from first incision to the time the patient was removed.
Using the data obtained from the sound level meter and the surgery logs, sound levels for each surgery were calculated. In particular, we monitored the average sound level during the surgery, as well as the peak sound pressure level observed during the period. The Table shown below gives the sound pressure level averaged over all surgeries monitored in a particular division and the range of average sound pressure levels for the surgeries. This is a tighter distribution of levels than anticipated and suggests that the prior literature might be overstating differences between types of surgeries as a result of the lack of a consistent measuring system. Further, it is clear from Table I that there is no discernable pattern that distinguishes the noisiest from the least noisy surgeries. For example, pediatric orthopedic surgery was the lowest level on average, but adult orthopedics, which uses the same procedures and instruments, was among the highest sound levels observed. These average sound levels resemble those one would expect about 100 meters from a busy highway or in a busy restaurant.
|
Division
|
No. of Surgeries
|
Ave. Level
dB(A)
|
Range
dB(A)
|
|
Pediatric Orthopedic
|
2
|
57.9
|
56.8 58.7
|
|
Gynecological
|
2
|
60.2
|
54.4 63.4
|
|
Thoracic
|
4
|
62.9
|
61.6 63.6
|
|
Gastrointestinal
|
9
|
62.9
|
54.9 - 68.8
|
|
Cardiology
|
10
|
63.4
|
57.1 67.8
|
|
Urology
|
11
|
63.6
|
55.6 67.0
|
|
Pediatric Urology
|
2
|
64.1
|
64.0 64.1
|
|
Neurosurgery
|
8
|
64.5
|
60.2 67.3
|
|
Otoloaryngology
|
4
|
64.8
|
53.0 66.4
|
|
Pediatric Plastic
|
4
|
65.2
|
62.2 68.4
|
|
Orthopedic
|
19
|
66.3
|
56.7 70.3
|
|
Plastic
|
3
|
66.9
|
58.8 68.9
|
The figure below shows the range of peak sound pressure levels observed in the operating room by surgical type. For each surgery, the peak sound pressure level was defined as the top value monitored by the sound level meter on the peak setting.
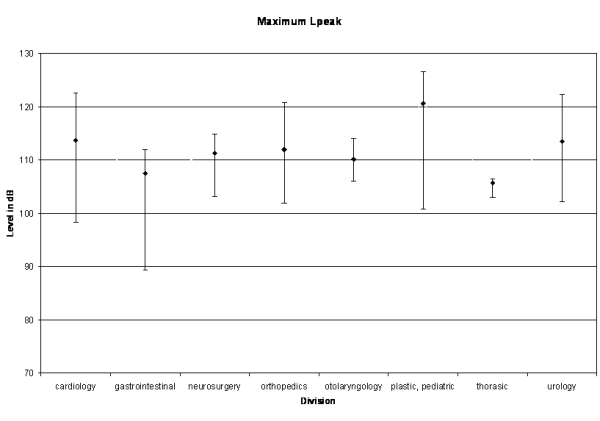
From this work, we conclude that surgery is a noisy business. Gastrointestinal and thoracic surgery are relatively quiet among the surgical divisions. Neurosurgery and orthopedics have sustained high sound levels. Cardiology surgery has a more moderate average sound level but includes brief periods of extremely high peak sound levels. There is no indication that the sound pressure levels found in the operating room are sufficiently high to cause hearing damage to patients. However, surgical staff is routinely exposed to these high noise levels and there is some likelihood that it will cause a cumulative degradation of hearing in these professionals. Also, it is likely that the noise in the operating room significantly degrades speech communication, a worry given the need for clear oral communication between members of the surgical team.
[ Lay Language Paper Index | Press Room ]