University of California, Irvine, Irvine, CA, 92697-5310, United States
Matthew Richardson and Harrison Lin
University of California, Irvine
Robert Carlyon
University of Cambridge
Popular version of 2aPP6 – Temporal pitch processing in an animal model of normal and electrical hearing
Presented at the 184 ASA Meeting
Read the abstract at https://doi.org/10.1121/10.0018352
A cochlear implant can restore reasonable speech perception to a deaf individual. Sensitivity to the pitches of sounds, however, typically is negligible. Lack of pitch sensitivity deprives implant users of appreciation of musical melodies, disrupts pitch cues that are important for picking out a voice amid competing sounds, and impairs understanding of lexical tones in tonal languages (like Mandarin or Vietnamese, for example). Efforts to improve pitch perception by cochlear-implant users could benefit from studies in experimental animals, in which the investigator can control the history of deafness and electrical stimulation and can evaluate novel implanted devices. We are evaluating cats for studies of pitch perception in normal and electrical hearing.
We train normal-hearing cats to detect changes in the pitches of trains of sound pulses – this is “temporal pitch” sensitivity. The cat presses a pedal to start a pulse train at a particular base rate. After a random delay, the pulse rate is changed and the cat can release the pedal to receive a food reward. The range of temporal pitch sensitivity by cats corresponds well to that of humans, although the pitch range of cats is shifted somewhat higher in frequency in keeping with the cat’s higher frequency range of hearing.
We record small voltages from the scalps of sedated cats. The frequency-following response (FFR) consists of voltages originating in the brainstem that synchronize to the stimulus pulses. We can detect FFR signals across the range of pulse rates that is relevant for temporal pitch sensitivity. The acoustic change complex (ACC) is a voltage that arises from the auditory cortex in response to a change in an ongoing stimulus. We can record ACC signals in response to pitch changes across ranges similar to the sensitive ranges seen in the behavioral trials in normal-hearing cats.
We have implanted cats with devices like cochlear implants used by humans. Both FFR and ACC could be recorded in response to electrical stimulation of the implants.
The ACC could serve as a surrogate for behavioral training for conditions in which a cat’s learning might not keep up with changes in stimulation strategies, like when a cochlear implant is newly implanted or a novel stimulating pattern is tested.
We have found previously in short-term experiments in anesthetized cats that an electrode inserted into the auditory (hearing) nerve can selectively stimulate pathways that are specialized for transmission of timing information, e.g., for pitch sensation. In ongoing experiments, we plan to place long-term indwelling electrodes in the auditory nerve. Pitch sensitivity with those electrodes will be evaluated with FFR and ACC recording. If performance of the auditory nerve electrodes in the animal model turns out as anticipated, such electrode could offer improved pitch sensitivity to human cochlear implant users.
Archie’s Cochlear Implant Laboratory, The Hospital for Sick Children, University of Toronto, The Hospital for Sick Children, TORONTO, ON, M5G1X8, Canada
Popular version of 3aPP5 – Non-auditory processing of cochlear implant stimulation after unilateral auditory deprivation in children
Presented at the 184 ASA Meeting
Read the abstract at https://doi.org/10.1121/10.0018669/
Decades of research have shown that hearing from only one ear in childhood should not be dismissed as a “minimal” hearing problem as it can impair language, cognitive, and academic development. We have been exploring whether there are effects of unilateral hearing on the developing brain. A series of studies has been done in children who have one deaf ear and who hear from the other side through a normal or typically hearing ear, a hearing aid, or a cochlear implant. We record electrical fields of brain activity from electrodes placed on the surface of the head (encephalography); we then calculate what parts of the brain are responding.
The findings show that auditory pathways from the hearing ear to the auditory cortices are strengthened in children with long term unilateral hearing. In other words, the hearing brain has developed a preference for the hearing ear. As shown in Figure 1, responses from the better hearing ear were also from areas of the brain involving attention and other sensory processing. This means that areas beyond the auditory parts of the brain are involved in hearing from the better ear.
Figure 1 legend: Cortical areas abnormally active from the experienced ear in children with long periods of unilateral cochlear implant use include left frontal cortex and precuneus.Adapted from Jiwani S, Papsin BC, Gordon KA. Early unilateral cochlear implantation promotes mature cortical asymmetries in adolescents who are deaf. Hum Brain Mapp. 2016 Jan;37(1):135-52. doi: 10.1002/hbm.23019. Epub 2015 Oct 12. PMID: 26456629; PMCID: PMC6867517.
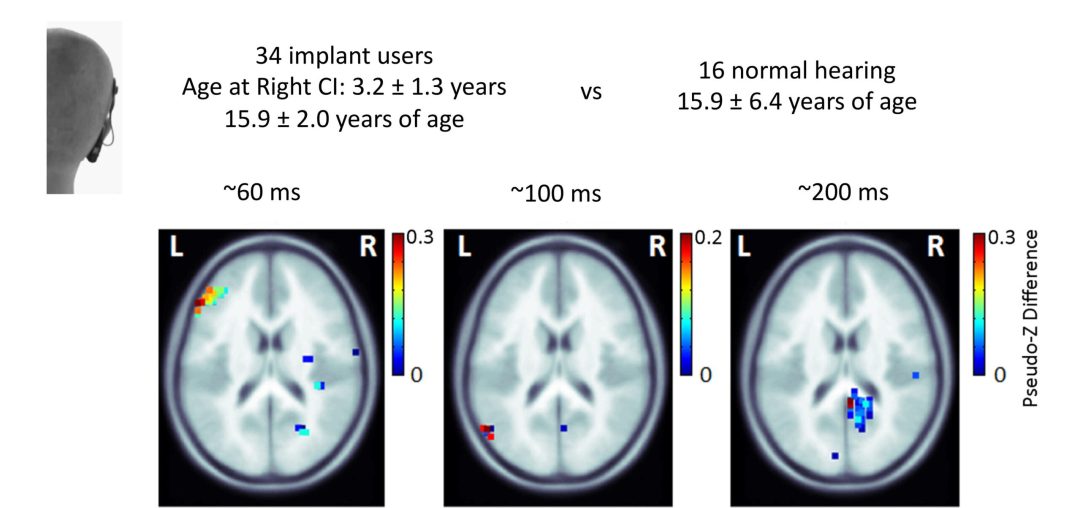
We also asked whether there were brain changes from the ear deprived of sound in children. This question was addressed by measuring cortical responses in three cohorts of children with unilateral hearing who received a cochlear implant in their deaf ear (single sided deafness, bilateral hearing aid users with asymmetric hearing loss, and unilateral cochlear implant users). Many of these children showed atypical responses from the cochlear implant with unusually strong responses from the brain on the same side of the deaf implanted ear. As shown in Figure 2, this unusual response was most clear in children who had not heard from that ear for several years (Figure 2A) and was already present during the first year of bilateral implant use (Figure 2B).
Figure 2 legend: Cortical responses evoked by the second cochlear implant (CI-2) in children receiving bilateral devices. A) Whereas expected contralateral lateralization of activity is evoked in children with short periods of unilateral deprivation/short delays to bilateral implantation, abnormal ipsilateral responses are found in children with long periods of unilateral deprivation despite several years of bilateral CI use. Adapted from: Gordon KA, Wong DD, Papsin BC. Bilateral input protects the cortex from unilaterally-driven reorganization in children who are deaf. Brain. 2013 May;136(Pt 5):1609-25. doi: 10.1093/brain/awt052. Epub 2013 Apr 9. PMID: 23576127. B) Abnormal ipsilateral responses are also found throughout the first year of bilateral CI use in children with long periods of unilateral deprivation/long delays to bilateral CI. Adapted from Anderson CA, Cushing SL, Papsin BC, Gordon KA. Cortical imbalance following delayed restoration of bilateral hearing in deaf adolescents. Hum Brain Mapp. 2022 Aug 15;43(12):3662-3679. doi: 10.1002/hbm.25875. Epub 2022 Apr 15. PMID: 35429083; PMCID: PMC9294307
New analyses have shown that this this response from the CI in the longer deaf ear includes areas of the brain involved in attention, language, and vision.
Results across these studies demonstrate brain changes that occur in children with unilateral hearing/deprivation. Some of these changes happen in the auditory system but others involve other brain areas and suggest that multiple parts of the brain are working when children listen with their cochlear implants.
Department of Otorhinolaryngology, Head and Neck Surgery Unversity of Zurich Frauenklinikstrasse 24 Zürich, 8091, SWITZERLAND
Cochlear Technology Centre Schalienhoevedreef 20 I Mechelen, 2800, BELGIUM
Cochlear AG Peter Merian-Weg 4 Basel, 4052, SWITZERLAND
Popular version of paper 2aEA6, “A MEMS condenser microphone based acoustic receiver for totally implantable cochlear implants” Presented Tuesday morning, May 8, 2018, 11:00-11:20 AM, Greenway D 175th ASA Meeting, Minneapolis
In the totally implantable cochlear implant (TICI) system, the external parts of the currently available cochlear implants (CIs) are integrated into the implant and hence, become invisible and well protected. Recipients using such a system would significantly benefit from 24/7 hearing and the overall improved quality of life that comes with an invisible hearing aid (related to playing sports, sleep comfort, reduced social stigma, etc.). A TICI system is not commercially available to date, mainly because of technical difficulties of making an implantable microphone (IM).
In contrast to an external microphone, an implantable one needs sophisticated packaging to meet stringent requirements for long term biocompatibility, safety and reliability. In addition, high sensing performance, low power consumption and simple surgical approach have to be considered during the design phase.
The goal of the present project is to develop and validate an IM for a TICI system.
Figure 1. Schematic drawing of the present concept of an IM for a TICI system. The illustration shows the main parts of the intracochlear acoustic receiver (ICAR) and their anatomical locactions. The sound receptor (SR) with up to 4 sound receiving protective diaphragms, the enclosure of the MEMS condenser microphone (CMIC) and the system for static pressure equalization (SPEQ) form a biocompatible Ti packaging structure which hermetically seals the MEMS CMIC against body tissue. The SPEQ system represents a passive adaptive volume which compensates for ambient static pressure variations and thus, provides stable sensing performance.
Our approach for an IM is a device which measures the pressure fluctuations in the cochlea (inner ear), which are induced by the outer and middle ear chain, a so-called intracochlear acoustic receiver (ICAR, Fig. 1). An ICAR benefits from the amplification and directionality cues of the ear anatomy, whilst minimizing interference by body noises. The ICAR might potentially be integrated into the existing CI electrode array and hence, such a TICI may benefit from a similar surgical procedure as applied for a CI.
The design concept for the ICAR is based on a commercially available MEMS condenser microphone (MEMS CMIC) as it is used for telecommunication devices. The MEMS CMIC of the ICAR is fully packaged in a biocompatible enclosure made out of titanium (Ti) but still enables sensing of the pressure fluctuations in the cochlea. The sensing capability of the MEMS CMIC is maintained by sealing its pressure sensing port with thin protective Ti diaphragms (PD). Sound induced vibrations of the PDs cause pressure fluctuations within the gas-filled volume formed by the PDs and the sensing element of the MEMS CMIC. Since the size of the MEMS CMIC enclosure prevents its insertion into the cochlea, only the thin sensor head carrying the PDs, called the sound receptor (SR), is inserted into the cochlea duct. The enclosure remains in the middle ear cavity adjacent to the entrance of the cochlea (Fig. 1).
Figure 2. The first prototype (PT I) of the proposed design concept of the ICAR (a). PT I uses a commercially available MEMS CMIC in its original packaging (c, top enclosure removed). An acrylic adapter interconnects the pressure port of the MEMS CMIC and the SR (fused silica capillary tube). The PD, a 1 micron thick polyimide diaphragm supported by a thin-wall cylindrical structure made out of single crystal silicon, seals the front end of the SR tube (b).
The development process of the ICAR started with a simplified version of the proposed concept. The first prototype (PT I) is not implantable and does not meet the sensing performance targeted in the final ICAR (Fig. 2). It was mainly designed to validate lumped element modelling of the sensor concept and to measure and quantify intracochlear sound pressure (ICSP) in human and sheep temporal bones, providing crucial information towards an ICAR of a TICI system [1, 2]. The data from ICSP measurements were in good agreement with results in the literature [3].
Figure 3. Prototype II (PT II) combines the SR from PT I and a custom-made Ti enclosure for the MEMS CMIC with optimum form factor for surgical insertion (b). The flexible interface between microphone and the amplifier unit simplifies surgical insertion and sensor fixation (a). A flexible printed circuit board (FCB) enables packaging of the MEMS CMIC and the corresponding ASIC unit in an enclosure with optimum form factor. In addition, it simplifies electrical interfacing due to an integrated FCB cable (c).
As the next step, the second ICAR prototype (PT II) was designed and built such that surgical insertion into the cochlea was possible during acute large animal experiments. In PT II, a custom-made Ti enclosure for the MEMS CMIC was combined with the SR of PT I (Fig. 3). A flexible interface between the microphone and the external amplifier unit allows surgeons to insert and fix the sensor without using complex assisting tools (e.g. micro-manipulator). The acute large animal experiments revealed that the presented ICAR concept is a suitable receiver technology for TICI systems.
Figure 4. CAD model of prototype III (PT III) of the ICAR combining the MEMS CMIC enclosure from PT II and a Ti SR with four 1 micron thick Ti diaphragms. The SR structure and the enclosure are laser welded together. The multi-diaphragm SR design is required to meet the targeted sensing performance (sensitivity, bandwidth). The micro-channel within the SR pneumatically interconnects the PDs and the MEMS CMIC.
Currently, a fully biocompatible ICAR (PT III, Fig. 4) is under development. PT III, which is planned to be used for chronic large animal tests, is expected to fulfill all requirements for application of the ICAR to a TICI system, including high performance, low power consumption and good system integration. The key feature of PT III is the Ti SR with four PDs instead of one as used in PT I and PT II. It is fabricated from thin Ti sheets which are structured by photo etching and hermetically joined by diffusion bonding. The 1 micron thick PDs are deposited onto the bare SR structure using DC magnetron sputtering on top of a low temperature decomposable polymer material (Fig. 5).
Figure 5. Tip region of the Ti SR of PT III after DC magnetron sputtering of a 1 micron thick Ti layer on both sides of the SR (picture from the first diaphragm fabrication trial on the multi-diaphragm SR structure design).
Acknowledgements This work was supported by the Baugarten Stiftung Zürich, Switzerland, by the Cochlear Technology Centre Belgium and by Cochlear AG, European Headquarters, Switzerland.
[1] F. Pfiffner, et al., “A MEMS Condenser Microphone-Based Intracochlear Acoustic Receiver” IEEE Transactions on Biomedical Engineering, 64, pp. 2431-2438, 2016
[2] D. Péus, et al., “Sheep as a large animal ear model: Middle-ear ossicular velocities and intracochlear sound pressure” Hearing research 351, pp. 88-97, 2017
[3] H. H. Nakajima, et al., “Differential intracochlear sound pressure measurements in normal human temporal bones” J Assoc Res Otolaryngol 10(1) pp. 23-36, 2009