Dr. rer. nat. Frank Wolfram Chirurgie II / Lung Cancer Centre SRH Wald-Klinikum Gera Straße des Friedens 122 07548 Gera Tel: 0365 82-83151 E-Mail: Frank.Wolfram@WKG.SRH.de
Presented Monday morning 10:40, May 13, 2019 177th ASA Meeting, Louisville, KY
Lung is known as a total acoustic absorber which in turn makes the use therapeutic ultrasound for local lung tumour treatment unsuitable.
By replacing pulmonary gas with saline, acoustic transmission can be achieved. Such One Lung Filling (OLF) has been studied intensively showing no cardio pulmonary deficiencies and is an accepted procedure in pneumology for clearance from proteinosis or silica dust.
Our aim is to combine OLF and therapeutic ultrasound where the cancerous lung is flooded while the contralateral side maintains ventilated. During stable OLF, central lung cancer tissue could be treated non-invasively using therapeutic ultrasound (HIFU). In order to understand ultrasound interaction in such flooded condition, the acoustic conditions were investigated and their impact on the lung cancer ablation process discussed.
For this study preclinical ex and in-vivo models have been used. Determination of acoustic parameter was performed using a broad band immersion technique. Lung cancers and flooded lung show a speed of sound and impedance as known solid tissue, whilst flooded lung show a significant lower attenuation. HIFU induces in adeno carcinoma temperatures above the ablative threshold (80°C), whilst the same acoustic dose in flooded lung only a non-lethal temperature rise (43°C) causes. Sonographic examinations revealed complete visibility of lung cancer and lung metastases.
During OLF atypical, but superior acoustic conditions for application of therapeutic ultrasound exists. Sonography is an excellent guiding modality providing a 100% tumor demarcation. The HIFU interacts with the malignant tissue leaving healthy lung parenchyma unaffected.
These findings suggest valuable benefits for future clinical implementation. Most lung cancer are inoperable at diagnosis due to poor lung function or advanced stage, the parenchyma sparing property of Lung HIFU could help to reduce tumor load while preserving lung function without toxicity. Additionally, the repeatability of therapeutic ultrasound can provide iterative treatment in case of recurrence or new metastasis.
Department of Information Engineering and Computer Science University of Trento, Italy
Popular version of paper 1pBA4 Presented Monday morning, May 13, 2019 177th ASA Meeting, Louisville, KY
Lung diseases have a large impact worldwide. Chronic Obstructive Pulmonary Diseases (COPD) and lower respiratory infections are respectively the third and fourth leading cause of death in the world, and are responsible for six million deaths per year [1]. Pneumonia, an inflammatory condition of the lung, is the leading cause of death in children under five years of age and responsible for approximately 1 million deaths per year. The economical burden is also significant. Considering only COPD, in the United States of America, the sum of indirect and direct healthcare costs is estimated to be in the order of 50 billion dollars [2].
Cost effective and largely available solutions for the diagnosis and monitoring of lung diseases would be of tremendous help, and this is exactly the role that could be played by ultrasound (US) technologies.
Compared to the current standard, i.e., X-ray based imaging technologies like a CT-scan, US tech is in fact safe, transportable, and cost-effective. Firstly, being an ionizing-radiation-free modality, US is a diagnostic option especially relevant to children, pregnant women and patients subjected to repeated investigations. Secondly, US devices are easily transportable to patient’s site, also in remote and rural areas, and developing countries. Thirdly, devices and examinations are significantly cheaper as compared to CT or MRI, making US tech accessible to a much broader range of facilities, thus reaching more patients.
However, this large potential is today underused. The examination of the lung is in fact performed with US equipment conceptually unsuitable to this task. Standard US scanners and probes have been designed to visualize body parts (hart, liver, mother’s womb, the abdomen) for which the speed of sound can be assumed to be constant. This is clearly not the case for the lung, due to presence of air. As a consequence, it is impossible to correctly visualize the anatomy of the lung beyond its surface and, in most conditions, the only usable products of standard US equipment are images that display “signs”.
These signs are called imaging artifacts, i.e., objects that are present in the image but which are not physically present in the lung (see example in the Figures). These artifacts, for most of which we still do not know why exactly they appear in the images, carry diagnostic information and are currently used in the clinics, but can obviously only lead to qualitative and subjective analysis.
Example of standard ultrasound images with different artifacts: A-line artifacts, left, are generally associated with a healthy lung, while B-lines, on the right, correlate with different pathological conditions of the lung. The arrows on top indicate the location of the lung surface in the image, visualized as a bright horizontal line. Beyond this depth the capability of these images to provide an anatomical description of the lung is lost.
Moreover, their appearance in the image largely depends on the user and on the equipment. Clearly, there is much more that we can do. Can we correctly (see) visualize what we (hear) receive from the lung after insonification? Can we re-conceive US tech in order to adapt it to the specific properties of the lung?
Can we develop an ultrasound-based method which can support, in real time, the clinician in the diagnosis of the many different pathologies affecting the lung? In this talk, trying to answer to these questions, recently developed imaging modalities and signal processing techniques dedicated to the analysis of the lung response to ultrasound will be introduced and discussed. In particular, in-vitro and clinical data will be presented which show how the study of the ultrasound spectral features [3] could lead to a quantitative ultrasound method dedicated to the lung.
[1] Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000-2016. Geneva, World Health Organization; 2018.
[2] The clinical and economic burden of chronic obstructive pulmonary disease in the USA, A.J. Guarascio et al. Clinicoecon Outcomes Res, 2013.
[3] Determination of a potential quantitative measure of the state of the lung using lung ultrasound spectroscopy. L. Demi et al. Scientific Reports, 2017.
Thomas Matula – matula@uw.edu Univ. of Washington 1013 NE 40th St. Seattle, WA 98105
Oleg A. Sapozhnikov Ctr. for Industrial and Medical Ultrasound Appl. Phys. Lab Univ. of Washington Seattle, Washington Phys. Faculty
Lev Ostrovsky Dept. of Appl. Mathematics University of Colorado Inst. of Appl. Phys. Russian Acad. of Sci. Boulder, CO
Andrew Brayman John Kucewicz Brian MacConaghy Dino De Raad Univ. of Washington Seattle, WA
Popular version of paper 2aBAb2 Presented Tuesday morning, Nov 6, 2018 176th ASA Meeting, Victoria, BC, Canada
Cells are isolated and sorted for a variety of diagnostic (e.g., blood tests) and therapeutic (e.g., stem cells, immunotherapy) applications, as well as for general research. The workhorses in most research and commercial labs are fluorescently-activated cell sorters (FACS) [1] and magnetically-labeled cell sorters (MACS) [2]. These tools use biochemical labeling to identify and/or sort cells which express specific surface markers (usually proteins). FACS uses fluorophores that target specific cell markers. The detection of a specific fluorescence wavelength tells the system to sort those cells. FACS is powerful and can sort based on several different cellular markers. However, FACS is also very expensive and complicated such that they are mostly found only in large core facilities.
MACS uses magnetic beads that attach to cell markers. Permanent magnets can then be used to separate magnetically-tagged cells from untagged cells. MACS is much less expensive than FACS, and can be found in most labs. However, MACS also suffers from weaknesses, such as low throughput, and can only sort based on a single marker.
We describe a new method that merges biochemical labeling with ultrasound-based separation. Instead of lasers and fluorophore tags (i.e., FACS), or magnets and magnetic particle tags (i.e., MACS), our technique uses ultrasound and microbubble tags (Fig. 1). Like FACS and MACS, we attach a biochemical label (an antibody) to attach a microbubble to the cell’s surface protein. We then employ an ultrasound pulse that generates an acoustic radiation force, pushing the microbubbles; the attached cells are dragged along with the microbubbles, effectively separating them from untagged cells. This is accomplished because cells only very lightly interact with ultrasound, whereas microbubbles interact very significantly with the sound waves. We theorized that the force acts on the microbubble while the cell acts as a fluid that adds a viscous drag to the system (see [3]).
Figure 1. Cell separation technologies
We can break down our studies into two categories, cell rotation and cell sorting. In both cases we constructed an apparatus to view cells under a microscope. Figure 2 shows a cell rotating as the attached microbubbles align with the sound field (the movie can be found by clicking here). We developed a theory to describe this rotation, and the theory fits the data well, allowing us to ‘measure’ the acoustic radiation force on the conjugate microbubble-cell system (Fig. 3).
Figure 2. A leukemia cell has two attached microbubbles. An ultrasound pulse from above causes the cell to rotate.
Figure 3. We assume that the microbubbles act as point forces. The projection of these forces perpendicular to the radiation force direction leads to a torque on the cell, which is balanced by the viscous torque. This leads to an equation of motion that can be put in terms of angular displacement. Thus, the parameters are detailed in [3]. The results are plotted along with the data, showing a nice match between the theory and data. For our conditions, the acoustic radiation force was found to be F=1.7×10-12N.
[IMAGE MISSING]
When placed in a flow stream with other cells, the tagged cells can be easily pushed with ultrasound. Figure 4a shows how a single leukemia cell is pushed downward while normal erythrocytes (red blood cells) continue flowing in the stream (the movie can be found by clicking here). This shows that one can effectively separate tagged cells. However, in a commercial setting, one wants to sort with a much higher concentration of cells. Figure 4b illustrates that this can be accomplished with our simple setup (the movie can be found by clicking here).
To summarize, we show preliminary data that supports the notion of developing an ultrasound-based cell sorter that has the potential for high throughput sorting at a fraction of the cost of FACS.
(a) [IMAGE MISSING]
(b) [IMAGE MISSING]
Figure 4. (a) A single leukemia cell is pushed downward by an acoustic force while red blood cells continue to flow horizontally. It should be possible to detect rare cells using this technique. (b) For high-throughput commercial sorting, a much larger concentration of cells must be evaluated. Here, a large concentration of red blood cells, along with a few leukemia cells are analyzed. The ultrasound pushes the tagged leukemia cells downward. We used blue for horizontal flow (red blood cells) and red for ultrasound-based forcing downward.
[1] M. H. Julius, T. Masuda, and L. A. Herzenberg, “Demonstration That Antigen-Binding Cells Are Precursors of Antibody-Producing Cells after Purification with a Fluorescence-Activated Cell Sorter,” P Natl Acad Sci USA 69, 1934-1938 (1972).
[2] S. Miltenyi, W. Muller, W. Weichel, and A. Radbruch, “High-Gradient Magnetic Cell-Separation with Macs,” Cytometry 11, 231-238 (1990).
[3] T.J. Matula, et al, “Ultrasound-based cell sorting with microbubbles: A feasibility study,” J. Acoust. Soc. Am. 144, 41-52 (2018).
Popular version of paper 1aBA5 Presented Monday morning, November 5, 2018 176th ASA Meeting, Minneapolis, MN
A key gap for underserved communities around the world is the lack of clinical laboratories and specialists to analyze samples. But thanks to advances in machine learning, a new generation of ‘smart’ point-of-care diagnostics are filling this gap and, in some cases, even surpassing the effectiveness of specialists at a lower cost.
Take the case of pneumonia. Left untreated, pneumonia can be fatal. The leading cause of death among children under the age of five, pneumonia claims the lives of approximately 2,500 a day – nearly all of them in low-income nations.
To understand why, consider the differences in how the disease is diagnosed in different parts of the world. When a doctor in the U.S. suspects a patient has pneumonia, the patient is usually referred to a highly-trained radiologist, who takes a chest X-ray using an expensive machine to confirm the diagnosis.
Because X-ray machines and radiologists are in short supply across much of sub-Saharan Africa and Asia and the tests themselves are expensive, X-ray diagnosis is simply not an option for the bottom billion. In those settings, if a child shows pneumonia symptoms, a cough and a fever, she is usually treated with antibiotics as a precautionary measure and sent on her way. If, in fact, the child does not have pneumonia, this means she receives unnecessary antibiotics, leaving her untreated for her real illness and putting her health at risk. The widespread overuse of antibiotics also contributes to the buildup in resistance of the so-called “superbug” – a global threat.
In this context, an interdisciplinary team of algorithm developers, software engineers and global health experts at Intellectual Ventures’ Global Good—a Bill and Melinda Gates-backed technology fund that invents for humanitarian impact—considered the possibility of developing a low-cost tool capable of automating pneumonia diagnosis.
The team turned to ultrasound – an affordable, safe, and widely-available technology that can be used to diagnose pneumonia with a comparable level of accuracy to X-ray.
It wouldn’t be easy. To succeed, the device would need to be cost-effective, portable, easy-to-use and able to do the job quickly, accurately and automatically in challenging environments.
Global Good started by building an algorithm to recognize four key features associated with lung conditions in an ultrasound image – pleural line, B-line, consolidation and pleural effusion. This called for convolutional neural networks (CNNs)—a machine learning method well-suited for image classification tasks. The team trained the algorithm by showing it ultrasound images collected from over 70 pediatric and adult patients. The features were annotated on the images by expert sonographers to ensure accuracy.
Figure 1: Pleural line (upper arrow) and a-lines (lower arrow), indication of normal lung
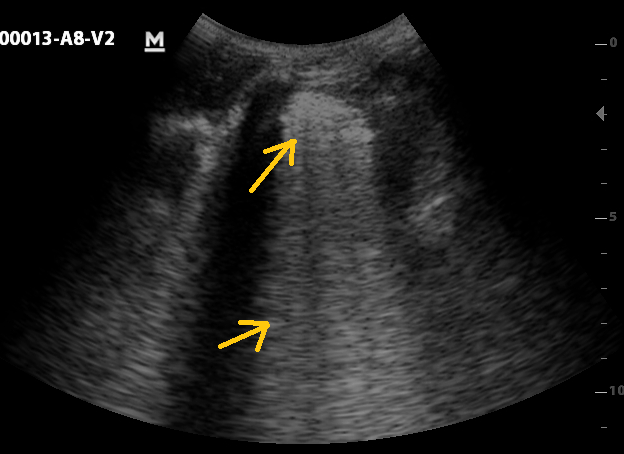
Figure 2: Consolidation (upper arrow) and merged B-line (lower arrow), indication of abnormal lung fluid and potentially pneumonia
Early tests show that the algorithm can successfully recognize abnormal lung features in ultrasound images and those features can be used to diagnose pneumonia as reliably as X-ray imaging—a highly encouraging outcome.
The algorithm will eventually be installed on an ultrasound device and used by minimally-trained healthcare workers to make high-quality diagnosis accessible to children worldwide at the point of care. Global Good hopes that the device will eventually bring benefits to patients in wealthy markets as well, in the form of a lower-cost, higher quality and faster alternative to X-ray.
Jonathan Mamou – jmamou@riversideresearch.org Daniel Rohrbach Lizzi Center for Biomedical Engineering, Riverside Research, New York, NY, USA
Sally A. McFadden – sally.mcfadden@newcastle.edu.au Vision Sciences, Hunter Medical Research Institute and School of Psychology, Faculty of Science, University of Newcastle, NSW, Australia
Quan V. Hoang – donny.hoang@snec.com.sg Department of Ophthalmology, Columbia University Medical Center, New York, NY USA Singapore Eye Research Institute, Singapore National Eye Centre, DUKE-NUS, Singapore
Myopia, or near-sightedness, affects up to 2.3 billion people and has a high prevalence. Although minimal levels of myopia are considered a minor inconvenience, high myopia is associated with sight-threatening pathology in 70% of patients and is highly prevalent in East Asians. By 2050, an estimated one billion people will have high myopia. High-myopia patients are prone to developing “pathologic myopia”, in which a high likelihood of permanent vision loss exists. Myopia is caused by an excessive eye length for the focusing power of the eye. Pathologic myopia occurs at extreme levels of lifelong, progressive eye elongation and subsequent thinning of the eye wall (sclera) and development of localized outpouchings (staphyloma). A breakdown in the structural integrity of the eye wall likely underlies myopic progression and precedes irreversible vision loss.
The guinea pig is a well-established animal model of myopia. With imposed blurring of the animals vision early in life, guinea pigs experience excessive eye elongation and develop high myopia within a week, which leads to pathologic myopia within 6 weeks. Therefore, we investigated two, fine-resolution ultrasound-based approaches to better understand and quantify the microstructural changes occurring in the posterior sclera associated with high-myopia development. The first approach termed quantitative-ultrasound (QUS) was applied to intact ex-vivo eyeballs of myopic and control guinea-pig eyes using an 80-MHz ultrasound transducer (Figure 1).
QUS yields parameters associated with the microstructure of tissue and therefore is hypothesized to provide contrast between control and myopic tissues. The second approach used a scanning-acoustic-microscopy (SAM) system operating at 250 MHz to form two-dimensional maps of acoustic properties of thin sections of the sclera with 7-μm resolution (Figure 2).
Like QUS, SAM maps provide striking contrast in the mechanical properties of control and myopic tissues at fine resolution. Initial results indicated that QUS- and SAM-sensed properties are altered in myopia and that QUS and SAM can provide new contrast mechanisms to quantify the progression and severity of the disease as well as to determine what regions of the sclera are most affected. Ultimately, these methods will provide novel knowledge about the microstructure of the myopic sclera that can improve monitoring and managing high myopia patients.
Michael Bailey – mbailey@uw.edu Center for Industrial and Medical Ultrasound Applied Physics Laboratory University of Washington 1013 NE 40th St. Seattle, WA 98105, USA apl.uw.edu/pushingstones
Popular version of paper 2pBAa1 Presented Tuesday afternoon 1:00 pm, November 6, 2018 176th ASA Meeting, Victoria BC
We are trying to change the way kidney stones are managed. Our solution is a painless, one-hour session where stones are identified, broken, and expelled from the kidney to pass naturally. This is an update on current progress to the doorstep of FDA clearance of an expelling system and first in human trials of a stone breaking system.
Stones are common and are currently managed in a long, costly, painful process. One in 11 Americans will have stones and cost of disease is $10B annually in the U.S. Stones are painful when they obstruct urine flow out of the kidney. Most people go to the Emergency Department where they to sent to a radiology department for a CT exam and then are given pain medication. They are expected to pass the stone within 3 weeks. If pain cannot be managed a surgery is performed to allow urine out of the kidney but not to remove the stone. If the first surgery has been performed, the stone is too large to pass or does not pass, or symptoms cannot be controlled, the patient has surgery to break the stone or stones usually with the expectation of the patient passing the fragments naturally. About one-third of surgeries leave fragments that can grow to again be symptomatic stones. Recurrence requiring intervention is about 50% within 5 years. Patients after the second stone event are usually monitored by CT annually for new stones. This process subjects patients to pain, anxiety, and ionizing radiation over a long time.
Our talk presents an update on our new non-invasive stone removal technology. We will present progress and results of several parallel clinical trials. Our NASA-funded study is to reposition an obstructing stone in the Emergency Department to relieve pain. One NIH-funded study is a randomized clinical trial to measure long term benefit of expelling fragments that remain after surgery. The status and design of studies to test the complete imaging, breaking and expelling technology will also be discussed. So far over 50 subjects are participating in the clinical trials.
We also will mention plans to improve the technology and further expand its use. This includes outputs to break stone faster based on image guided feedback of the progression of the individual’s specific procedure and stone characteristics. It also includes tractor beam technology to grab and steer stones and fragments through the complex three-dimensional path out of the kidney. Other talks in the session provide more detail on the development of these additional technologies.
Figure 1 shows a movie taken from a camera inside a patient’s kidney while the ultrasound sent from a probe on the patient’s skin causes an 4-mm (1/4 inch) kidney stone to move out of the kidney.
Figure 2 is a drawing of the new system and process.

 Lung is known as a total acoustic absorber which in turn makes the use therapeutic ultrasound for local lung tumour treatment unsuitable.
Lung is known as a total acoustic absorber which in turn makes the use therapeutic ultrasound for local lung tumour treatment unsuitable.