Using ultrasound as an antibody in Alzheimer’s and as a drug dose enhancer in cancer patients
Elisa Konofagou – ek2191@columbia.edu
Columbia University, 1210 Amsterdam Ave, New York, New York, 10027-7003, United States
Popular version of 2aBAa1 – Neuronavigated focused ultrasound for clinical bbb opening in alzheimer’s and brain cancer patients
Presented at the 184 ASA Meeting
Read the abstract at https://doi.org/10.1121/10.0018295
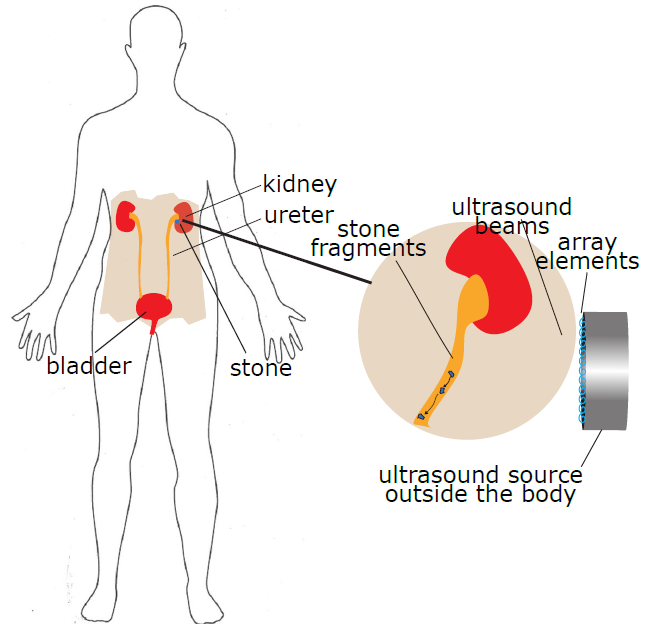
Ultrasound is widely known as an imaging modality in obstetrics and cardiology as well as several other applications but less known regarding its therapeutic effects despite its recent approvals in the clinic for ablation of prostate cancer and essential tremors. In the studies presented, we demonstrate that focused ultrasound (FUS) can be used in conjunction with microbubbles to open the blood-brain barrier (BBB) through the intact scalp of Alzheimer’s and pediatric tumor patients. The BBB is the main defense of the brain against toxic molecules but also prevents drugs from treating brain disease. In the case of Alzheimer’s, we demonstrate for the first time that the BBB opening resulting from FUS in the prefrontal cortex acts as an antibody in the brain. BBB opening results into a beneficial immune response in the brain that significantly reduces the beta amyloid in the region where ultrasound opened the blood-brain barrier. This was shown in 5 patients with Alzheimer’s.

In the case of the pediatric tumor patients, we aimed into the stem, which is a critical region between the spinal cord and the brain. The tumors in the pediatric patients are gliomas that grow in the stem where critical nerve fibers run through and they are therefore inoperable. We showed for the first time that BBB opening can be repeatedly induced with FUS in conjunction with microbubbles safely and efficiently in patients with pediatric glioma tumors in the stem. In this case, we used FUS in conjunction with a drug that, when crossing the blood-brain barrier, increases its efficiency. The patients reported smoother limb movement after treatment with the drug potentially acting more potently on the tumor.
It was concluded that ultrasound can safely open the blood-brain barrier in both patients as young as 6 years old to as old as 83 years old completely noninvasively and more importantly reduce the disease pathology and/or symptoms. The system is thus versatile, does not require a dedicated MR system or to be performed in the MR scanner unlike other systems and the entire procedure can last less than 30 min from start to finish. Ultrasound can thus be used alone or in conjunction with a drug in order to change the current dire landscape of treatment of brain disease. Finally, we show how Alzheimer’s beta amyloid and tau are excreted from the brain and can be detected with a simple blood test.